

Cancer Awareness & Oncology
The Pancreas Paradox: When “Normal” Health Checks Miss a Silent Killer
by Adj A/Prof Glenn Bonney, PanAsia Surgery
Pancreas model with awareness ribbon highlighting the silent risks of pancreatic cancer despite normal health screenings.
In the quiet, pressurised air of an operating theatre, I once reflected on a patient’s “clean bill of health.” Just two months earlier, every test result had come back normal. Yet I was about to operate again to remove a deadly disease.
Many people believe that a normal blood test or a clear ultrasound protects them. In reality, that belief can be misleading.
As a surgeon-scientist, I have treated many patients who were fit, disciplined, and proactive. Still, they were caught off guard by one of the most elusive organs in the body—the pancreas.
This is what I call the Pancreas Paradox: cancer can grow silently while the rest of the body appears healthy.
In Singapore, where health screening is common, pancreatic cancer remains a dangerous outlier. Standard tests can miss it.
The Stealth Nature of Pancreatic Cancer
Pancreatic cancer often hides until it reaches an advanced stage.
Even individuals with access to top medical care have fallen victim to it. The disease thrives because it remains undetected for long periods.
Well-known cases highlight this danger:
- Steve Jobs battled a pancreatic neuroendocrine tumour for years
- Patrick Swayze was diagnosed at Stage IV after mild symptoms
- Aretha Franklin fought a long, private battle
These cases show that pancreatic cancer does not discriminate. It can affect anyone, regardless of health status.
Rising Global and Local Trends
Close-up illustration of pancreatic cancer cells, representing one of the most aggressive and hard-to-detect cancers.
Pancreatic cancer cases are increasing worldwide.
Experts project that it will become the second leading cause of cancer death by 2030. By 2040, global cases may rise by about 70%.
In Singapore, the situation is also concerning:
- It is the fourth leading cause of cancer death
- About 80% of cases are diagnosed late
Symptoms like jaundice or back pain often appear too late. At that point, surgery may no longer be an option.
Advances in Surgery—But Limits Remain
Pancreatic surgery has improved significantly over the years.
Today, surgeons use robotic and minimally invasive techniques. These tools allow precise movement and faster recovery.
However, long-term outcomes remain challenging.
Even with successful surgery and chemotherapy, survival rates are still low. Surgery removes visible tumours, but microscopic cancer cells often remain aggressive.
Surgery is important—but it is not a complete cure.
Why the Pancreas Is So Hard to Detect

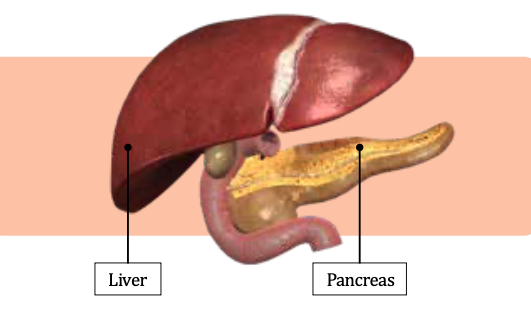
Medical visual of the pancreas location within the human body, emphasising its role in overall health.
The name of the organ originates from the Greek word pankreas (pan meaning “all,” and kreas meaning “flesh”). Ancient Greek physicians, led by Herophilus, viewed it as a protective cushion for the major abdominal vessels. Later, Claudius Galen described it as a pad to protect the spine – a functional misconception that persisted for a millennium and arguably hindered clinical research.
In Traditional Chinese Medicine, pancreatic function is often integrated into the “Spleen” system, regarded as the central pivot for the transformation of “Qi” and the regulation of metabolic harmony. This historical view of the pancreas as a biological “alchemist” is anatomically validated: situated deep behind the stomach and the spine, the organ regulates glucose metabolism through insulin and facilitates digestion via enzymes. Its deep- seated position is its primary defence, allowing tumours to develop entirely asymptomatically.
The Limits of Routine Screening
Many people rely on tumour markers like CA19-9 during health screenings.
However, this marker has major limitations:
- It may appear normal in early cancer
- It can rise due to non-cancer conditions like gallstones
Doctors mainly use CA19-9 to monitor known cancer—not to detect it early.
Standard ultrasounds also have limitations. Gas in the intestines can block a clear view of the pancreas.
More advanced imaging is often needed, such as:
- Specialised pancreatic MRI
- Photon-counting CT scans
These tools can detect small cysts and early changes that routine scans may miss.
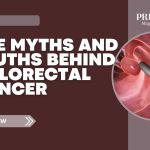
Anatomical illustration showing the liver and pancreas, key organs involved in digestion and metabolic health.
The Importance of Early Detection
Early detection offers the best chance of survival.
Doctors often look for precursor lesions, such as pancreatic cysts (e.g., IPMNs). These may appear incidentally during scans.
Managing these findings requires balance. Doctors must avoid unnecessary anxiety while ensuring serious risks are not overlooked.
Clinical guidelines, such as the Pan-Asian adapted ESMO framework, help doctors make consistent decisions. These guidelines provide a structured approach to diagnosis and follow-up.
The Future: Vaccine-Based Therapies
Researchers are exploring new ways to fight pancreatic cancer.
One promising area is cancer vaccines.
Some centres, like Memorial Sloan Kettering, are testing personalised mRNA vaccines. These are still in early stages and may be costly.
Another approach involves exosome-based vaccines. These use natural particles to deliver signals to the immune system.
Research at the National University of Singapore is studying how these vaccines can train the immune system to recognise cancer early.
While still experimental, these developments offer hope.
Rethinking “Normal” Health Results
In 2026, advances in surgery, imaging, and research are helping us better understand pancreatic cancer.
But one key message remains:
A “normal” health screening result does not guarantee safety.
The pancreas requires specialised attention. Detecting problems early often needs more than routine tests.
Being proactive means:
- Asking deeper questions
- Seeking specialist advice when needed
- Not relying solely on basic screening results
Awareness and early action remain our strongest tools against this silent disease. PRIME







Leave A Comment