

Heart Health & Preventive Cardiology
Think Your Cholesterol Is Normal? Think Again
By Dr Benji Lim, Senior Interventional Cardiologist, Novena Heart Centre
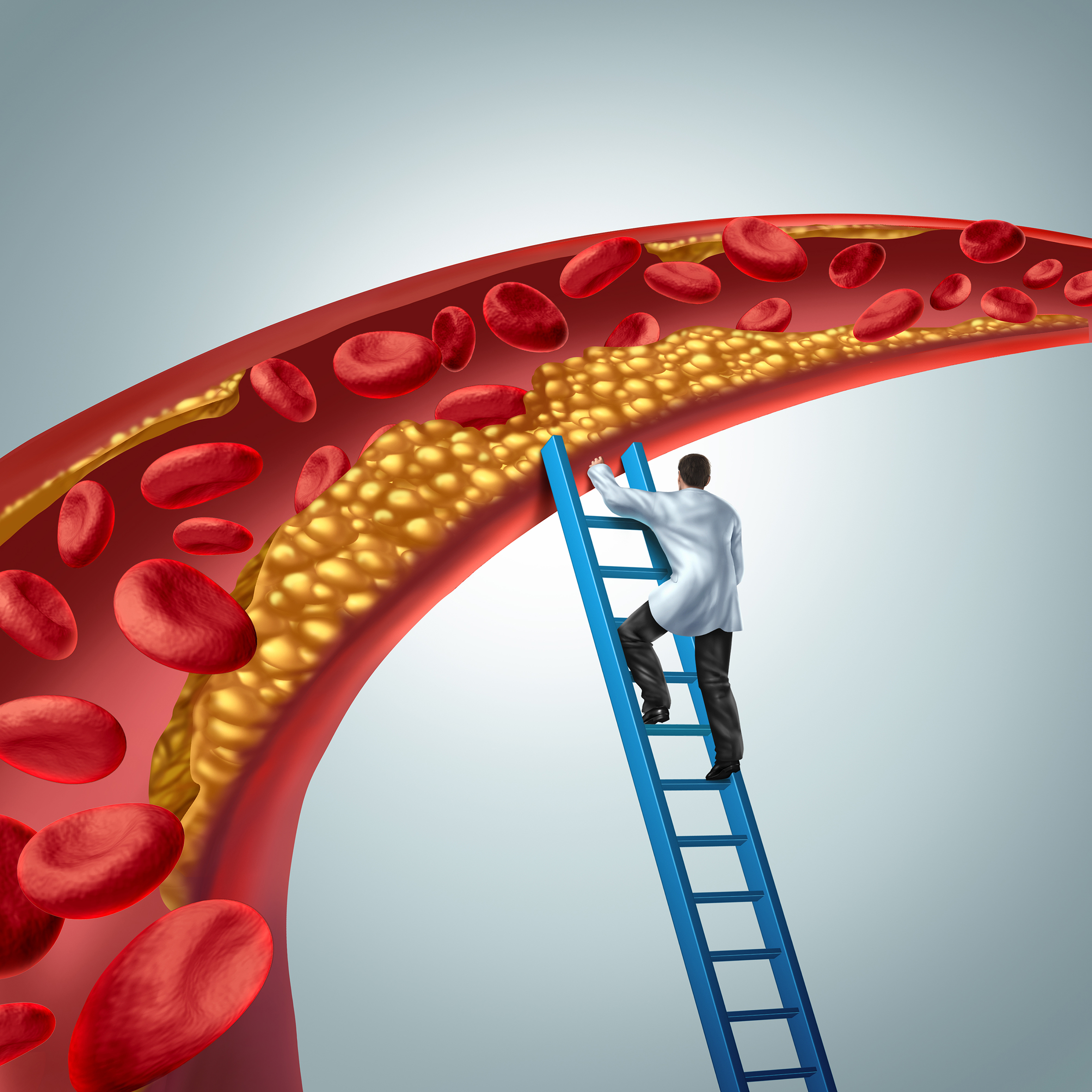
Cholesterol medical diagnosis concept as a doctor investigating atherosclerosis or arterial plaque clogging an artery with 3D render elements.
What Every Patient Needs to Know About Cholesterol and the Heart – An Interventional Cardiologist’s Perspective
As an interventional cardiologist, I spend much of my work inside the coronary (heart) arteries – opening blocked vessels, implanting stents, and treating heart attacks in real time. While these procedures can be lifesaving, the uncomfortable truth is that most of what I treat could have been prevented. Many people assume their results are safe, but what doctors call normal cholesterol risk may still carry hidden dangers. Many of my patients are shocked to learn that they have severe heart disease – they had felt perfectly well until the moment they suffered a heart attack.
In Singapore, 30% of all deaths are due to heart diseases or stroke, and there has been a 44% increase in the number of heart attack cases between 2012 to 2022. Ischaemic heart disease remains one of the leading causes of death, despite excellent access to healthcare and advanced medical technology.
At the centre of coronary artery disease lies one major culprit – cholesterol. Despite decades of public health messaging, many misconceptions still persist. Some people assume cholesterol is only a problem when symptoms appear, while others dismiss a “borderline” result as harmless. There is also a common belief that taking a statin alone eliminates all risk. In reality, cholesterol management is far more nuanced, especially when newer risk factors such as lipoprotein(a) are considered.
Cholesterol – Not All the Same
Cholesterol is a waxy, fat-like substance that is essential for life. It forms part of cell membranes, hormones, and bile acids. Because cholesterol does not dissolve in blood, the body transports cholesterol around by particles known as lipoproteins. The most important ones to understand are:
- Low-density lipoprotein (LDL): Often called “bad cholesterol”.
- High-density lipoprotein (HDL): Often referred to as “good cholesterol”.
- Triglycerides: A type of fat found in blood which increases the risk of heart disease.
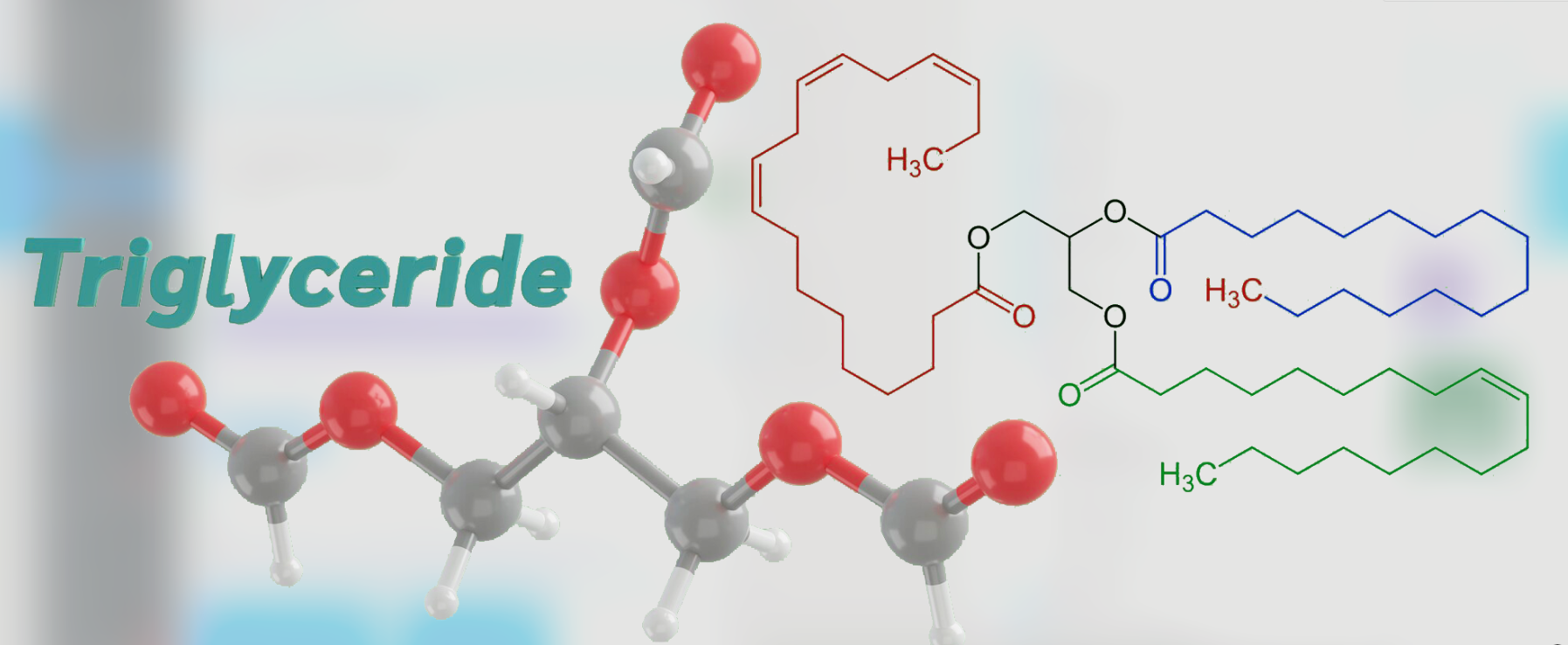
Triglyceride Molecule Structure and Its Role in Cardiovascular Risk
- Lipoprotein(a): A genetically determined and often overlooked risk factor.
Among these, LDL cholesterol is the primary driver of atherosclerosis, the process by which plaque builds up in the arteries.
Why LDL Cholesterol Matters So Much
When LDL cholesterol levels are high, LDL particles penetrate the inner lining of the arteries. Over time, these particles become oxidised and trigger inflammation. The body responds by sending immune cells to the area, gradually forming fatty plaques within the vessel wall.
As an interventional cardiologist, I often see the consequences of this process in the coronary arteries, including:
✅ Tight blockages which can become calcified or hardened.
✅ Long segments of diffuse narrowing.
✅ Sudden plaque rupture leading to heart attacks.
Importantly, cholesterol-related plaque builds up silently. Many patients feel completely well – until the day they do not. In fact, a heart attack is often the first symptom of coronary artery disease. Data from our local heart attack registry highlights this: one in seven Singaporeans did not experience any symptom before a heart attack.
“Normal” Cholesterol Is Not Always Safe
One of the most common questions I hear is: “Doctor, my cholesterol isn’t that high. Do I really need treatment?” The answer depends on overall cardiovascular risk, not just a single cholesterol number. Even so-called “normal” LDL may be too high if you have any of the following conditions:
- Established heart disease.
- Previous stroke.
- Peripheral artery disease (blockages in the leg arteries).
- Diabetes.
- Chronic kidney disease.
- Genetic causes of high cholesterol (e.g. familial hypercholesterolaemia).
- Very high LDL levels (i.e. above 4.9 mmol/L or 190 mg/dL).
- Multiple risk factors.
Current evidence shows that lower LDL is better, especially for people at moderate to high risk. Studies show that the risk of major cardiovascular events can be reduced by 20-25% per 1 mmol/L (or 39 mg/dL) reduction in LDL. In patients who already have coronary artery disease, evidence-based guidelines from major cardiology societies around the world recommend LDL levels well below what was previously considered acceptable, so as to prevent future cardiac events and lower overall cardiovascular risk.
HDL – The “Good” Cholesterol with Caveats
HDL cholesterol helps carry cholesterol away from the arteries and back to the liver. Higher HDL levels are generally associated with lower cardiovascular risk. However, raising HDL artificially with medications has not been shown to reduce heart attacks. This tells us that HDL is more of a risk marker than a direct treatment target. Lifestyle measures such as regular exercise, weight management, and smoking cessation remain the best ways to support healthy HDL levels.
Triglycerides – More Than Just a Number
Doctors commonly see elevated triglycerides in people with:
- Diets high in saturated fat, simple sugars, and caloric intake.
- Obesity.
- Poorly controlled diabetes.
- Metabolic syndrome.
- Excessive alcohol intake.
High triglyceride levels contribute to cholesterol particles that promote plaque build-up in the arteries (atherosclerosis). They are increasingly recognised as an independent cardiovascular risk factor. Addressing them often requires dietary changes, weight loss, better blood sugar control, and in some cases, medication.
Lipoprotein(a) – The Hidden Risk Factor
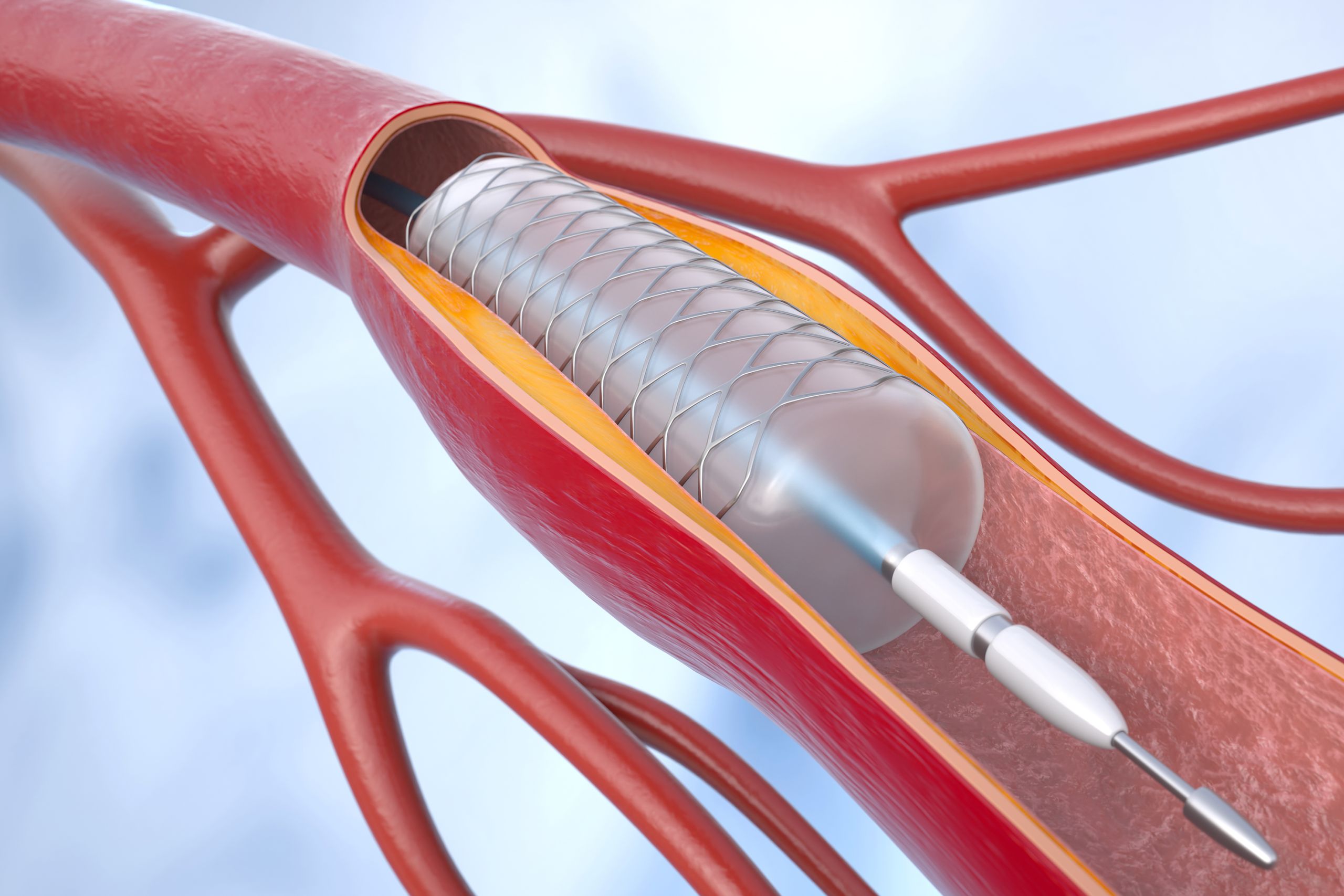
Coronary angioplasty with stenting (percutaneous coronary intervention or PCI) helps improve the blood supply to heart. 3D illustration
One of the most important and least understood cholesterol-related particles is lipoprotein(a), abbreviated as Lp(a). Lp(a) refers to a modified LDL particle with an additional apolipoprotein A protein attached. This protein makes Lp(a) particularly atherogenic and dangerous in two ways:
- It accelerates plaque formation in the arteries.
- It promotes blood clot formation.
Unlike LDL cholesterol, genetics largely determine Lp(a) levels, and these levels do not change significantly in adulthood.
What makes Lp(a) especially concerning is that:
- It can cause premature heart disease.
-
It often affects patients with few traditional risk factors.
-
It may explain heart attacks in people with “normal” cholesterol levels.
In my practice, I frequently encounter patients who suffer heart attacks in their 30s or 40s – some even in their late 20s – only to discover they have markedly elevated Lp(a).
Who Should Be Tested for Lipoprotein(a)?
Because Lp(a) is an independent risk factor for cardiovascular disease, many international cardiology societies now recommend that Lp(a) be measured at least once in a person’s lifetime, especially in those with:
-
A family history of early heart disease.
-
Heart attacks at a young age.
-
Recurrent cardiovascular events despite good LDL control.
When we identify elevated Lp(a), we can take a more aggressive approach with LDL lowering and risk factor modification.
Cholesterol Treatment – Beyond Statins
Statins remain the cornerstone of cholesterol management. They are safe, effective, and backed by decades of evidence showing reductions in heart attacks, strokes, and cardiovascular death. While they can cause side effects, such as muscle ache and liver dysfunction, most side effects are mild, while severe or clinically significant side effects are rare and occur in less than 1% of patients. In my daily practice, most patients who report side effects can continue statins safely with dose adjustment or a different formulation. Multiple large studies over decades have shown that the benefits of statin therapy in reducing mortality and cardiovascular events far outweigh the possible small risks of side effects.
However, statins are not the only tool we have. Depending on risk level and cholesterol response, other treatment options may include:
- Ezetimibe: Reduces cholesterol absorption from the gut.
- PCSK9 Inhibitors: Powerful injectable medications that can dramatically lower LDL and also reduce Lp(a) to some extent.
- Newer Therapies Targeting Lp(a) Directly: Currently in advanced clinical trials.
- Fibrates: Break down fat and reduce fat production in the liver, thus lowering triglycerides.
For high-risk patients, particularly those with established heart disease, combination therapy is often necessary to achieve guideline-directed optimal cholesterol targets.
Lifestyle Still Matters

Regular Walking for Heart Health and Cholesterol Control
No discussion about cholesterol is complete without addressing lifestyle. While genetics play a major role and only 20% of the cholesterol in our body comes from our diet, lifestyle choices can still significantly influence overall cardiovascular risk.
Key principles include:
- A diet rich in vegetables, fruits, wholegrains, and healthy fats.
- Limiting saturated fats, processed foods, and refined sugars.
- Regular physical activity and exercise.
- Maintaining a healthy body weight.
- Avoiding smoking.
- Limiting alcohol intake.
Making healthier choices at hawker centres and incorporating regular walking into daily routines can already make a meaningful difference. Lifestyle measures work best together with medication, not as a replacement when risk is high.
A Cardiologist’s Final Message
From the catheterisation laboratory, the message is clear: cholesterol matters long before symptoms appear. By the time a stent is needed, the disease process has been present for years. The goal of modern cardiology is not just to treat heart attacks, but to prevent the first one from happening. Understanding and managing cholesterol, including the lesser-known lipoprotein(a), in addition to other modifiable cardiovascular risk factors such as diabetes, high blood pressure, smoking, sedentary lifestyles, and unhealthy diets, allow us to identify risk earlier, personalise treatment, and most importantly save lives. Ultimately, cholesterol management is not about chasing a number – it is about protecting your future heart health. PRIME
Author

You Might Also Like:
 Silent Killer: Understanding Ischaemic Heart Disease by Dr Benji Lim
Silent Killer: Understanding Ischaemic Heart Disease by Dr Benji Lim
 Ischaemic Heart Disease Explained by Dr. Benji Lim | Novena Heart Centre
Ischaemic Heart Disease Explained by Dr. Benji Lim | Novena Heart Centre
 Do You Really Need a Heart Checkup? | Dr. Benji Lim Explains
Do You Really Need a Heart Checkup? | Dr. Benji Lim Explains
 Cholesterol Explained: Good vs Bad & How to Lower Your Risk | Dr. Benji Lim
Cholesterol Explained: Good vs Bad & How to Lower Your Risk | Dr. Benji Lim
 All Clear: Advancements in Coronary Angioplasty for the Treatment of Coronary Artery Disease by Dr Joshua Loh
All Clear: Advancements in Coronary Angioplasty for the Treatment of Coronary Artery Disease by Dr Joshua Loh




Leave A Comment