

Understanding Helicobacter pylori
Helicobacter pylori (HP) is a spiral-shaped bacterium commonly found in the human stomach and duodenum. It is estimated that up to half of the world’s population carries this infection. HP is especially common in developing countries.
For many years, doctors believed that stomach and duodenal ulcers resulted mainly from excessive stomach acid. Stress, smoking, and irregular meals were thought to be the main triggers. Classic surgical textbooks even described operations to treat ulcers by removing the acid-producing part of the stomach or cutting the nerves that control acid secretion.
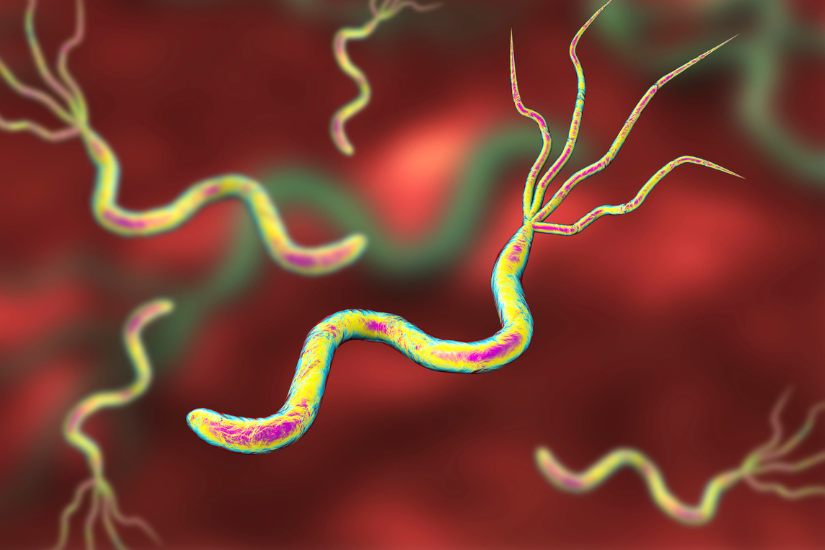
Helicobacter pylori: the hidden stomach bacterium behind ulcers, chronic gastritis, and increased cancer risk.
By the 1980s, medications such as acid blockers (for example, Zantac and Tagamet) became widely used. While these drugs helped ulcers heal, the problem often returned once treatment stopped.
The understanding of ulcers changed when Dr Barry Marshall and Dr Robin Warren demonstrated that a bacterium—HP—was the true cause. Their work initially faced strong resistance. To prove his point, Dr Marshall famously infected himself with HP, showing that it caused gastritis in a healthy person. This experiment, together with many clinical trials, eventually convinced the medical community that antibiotics could cure ulcers by eradicating HP. For their groundbreaking discovery, Marshall and Warren received the Nobel Prize in 2005.
HP Transmission
HP does not always cause disease. In some people, it lives in the stomach without producing any symptoms. Doctors cannot reliably predict who will develop problems, as both bacterial strain differences and individual susceptibility play a role.
Besides the stomach, HP can also be detected in saliva and stool. Infection usually spreads through oral-to-oral or faecal-to-oral contact. Most people acquire HP during childhood, often from contaminated food or water. Sharing food with infected individuals may also contribute to transmission, which may explain why HP is particularly common in Asia, where communal dining is common.

Poor sanitation and unsafe water are major risk factors for Helicobacter pylori infection.
Testing for HP
HP infection may cause symptoms such as bloating, indigestion, nausea, vomiting, upper abdominal discomfort, bad breath, and less commonly, diarrhoea. If your doctor suspects HP as the cause of your symptoms, testing and treatment with antibiotics may provide a cure.
Doctors also recommend HP testing if you have:
-
A history of stomach or duodenal ulcers
-
A need for long-term medications that increase ulcer bleeding risk, such as aspirin or non-steroidal anti-inflammatory drugs (NSAIDs) like naproxen
HP infection is frequently found in patients with stomach cancer. In 1994, the World Health Organization classified HP as a Class I carcinogen for gastric cancer. If you have a strong family history of stomach cancer, your doctor may advise testing and treating HP to reduce your future risk.
Methods of Testing
Testing for HP is simple and reliable.
Non-invasive tests include:
-
Urea Breath Test (UBT)
-
Stool antigen test
Blood tests that detect HP antibodies are available but not recommended. A positive result cannot distinguish between an active infection and a past one, as antibodies can remain positive for many years after treatment.

The Urea Breath Test offers a safe and accurate way to detect Helicobacter pylori without invasive procedures.
Urea Breath Test (UBT)
The UBT is a safe, non-invasive, and highly accurate test developed by Dr Marshall. It has a sensitivity and specificity of about 95%.
To prepare for the test:
-
Fast for at least 6 hours beforehand
-
Do not smoke for 6 hours before the test
-
Avoid antibiotics for 1 month and stomach acid medications for 1 week before testing
These medications may affect test accuracy.
During the test, you swallow a tablet containing 100 mg of urea labelled with a non-radioactive carbon-13 isotope. If HP is present, the bacterium breaks down the urea into ammonia and carbon dioxide. The carbon dioxide enters the bloodstream and is exhaled through the lungs. The laboratory detects the labelled carbon dioxide from a breath sample collected about 20 minutes later.

Gastroscopy is a procedure that helps doctors diagnose gastritis, ulcers, and Helicobacter pylori infection.
Gastroscopy
Doctors can also test for HP during a gastroscopy. During the procedure, they take small biopsies from the stomach lining. These samples are examined under a microscope or placed into a rapid urease test kit. If HP is present, the urea in the kit converts to ammonia, causing a visible colour change.
In cases of suspected antibiotic resistance, doctors can culture HP from biopsy samples. This allows testing of antibiotic sensitivity to guide further treatment.
Gastroscopy remains the gold standard for diagnosing HP when endoscopy is clinically indicated. It also allows direct visual assessment of the oesophagus, stomach, and duodenum.
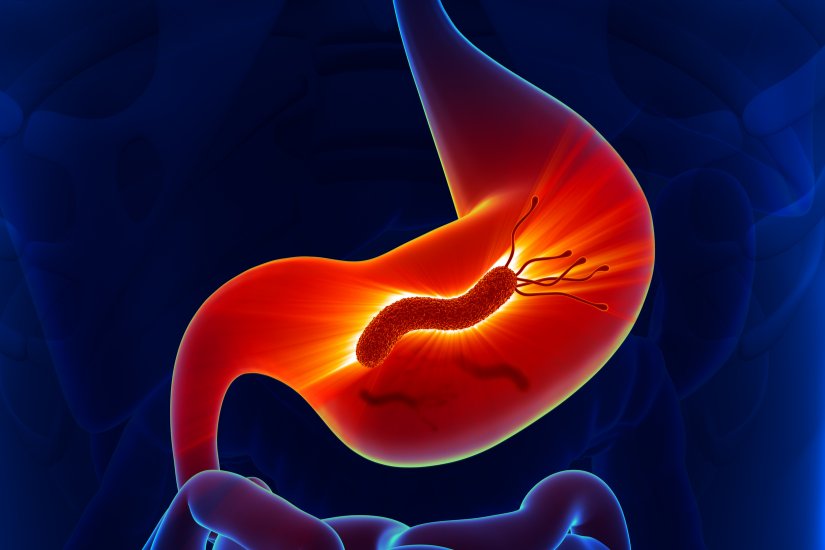
A visual illustration of Helicobacter pylori damaging the stomach lining and triggering inflammation.
Understanding Gastritis
Many people use the term “gastritis” to describe indigestion, bloating, or upper abdominal pain. Medically, however, gastritis refers specifically to inflammation of the stomach lining.
HP commonly causes gastritis, but other causes include excess acid, medications, alcohol, and smoking.
Doctors usually diagnose gastritis through gastroscopy. A healthy stomach lining appears pink and smooth, while gastritis may show redness, nodules, erosions, or irregular surfaces. Biopsy samples help confirm the diagnosis, with results typically available within a few days.
Gastroscopy can also detect ulcers, cancers, and pre-cancerous changes. Modern endoscopic techniques, such as magnification and chromoendoscopy, allow doctors to detect very early disease.
Early-stage stomach cancer is often curable. Identifying pre-cancerous changes, such as intestinal metaplasia, helps doctors identify patients who require closer surveillance. Treating HP reduces the overall risk of gastric cancer by eliminating its main causative factor.
Treatment of HP
Doctors only treat HP when testing confirms infection. Choosing the right treatment can be challenging. Most regimens require a combination of three or four medications, including antibiotics, acid-suppressing drugs, and sometimes probiotics. Patients usually take these medications several times a day for 10 to 14 days.
Because antibiotic resistance is increasing worldwide, treatment success rates average around 80%. Doctors usually recommend a Urea Breath Test 1 to 3 months after treatment to confirm eradication. If HP persists, a second or even third course of different antibiotics may be necessary.
Once treatment successfully eradicates HP, the risk of future reinfection remains very low. PRIME








Leave A Comment