

Common Liver Problems in Women’s Health
Liver health is vital for women’s overall well-being. The liver supports many essential processes: it breaks down nutrients, removes toxins, regulates blood sugar, and produces bile to digest fats.
Unfortunately, liver disorders are becoming more common in women. Many of these conditions can lead to serious complications if left untreated.
This article highlights some of the most common liver disorders in women and explains how they are diagnosed and managed.
Fatty Liver Disease
Case Example — Madam A
Madam A visited my clinic after a health screening ultrasound showed fatty liver and mildly abnormal liver tests. The finding surprised her. She believed fatty liver affected only certain body types.
Madam A works as an IT programmer and often stays up late for projects. She snacks at night, exercises infrequently because of work demands, and enjoys wine or beer on weekends. She weighs 66 kg, and her body mass index (BMI = weight/height²) is 26.
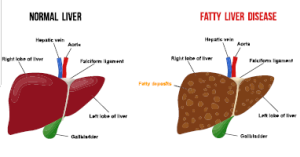
What Is Fatty Liver?
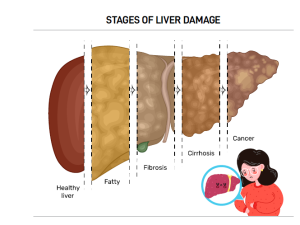
Fatty liver disease affects more than 30% of the population. It happens when the liver stores too much fat. A healthy liver contains only small amounts of fat, but when fat exceeds 5% of its weight, problems can occur.
The disease ranges from simple fat accumulation to inflammation and liver cell damage. Advanced cases may progress to cirrhosis, where scar tissue replaces healthy cells and may lead to liver cancer.
Types and Causes
-
Alcoholic fatty liver disease — caused by heavy alcohol intake.
-
Non-alcoholic fatty liver disease (NAFLD) — linked to metabolic issues such as higher body fat, type 2 diabetes, high blood pressure, and high cholesterol. Even moderate alcohol use can worsen NAFLD.
Lifestyle Changes for Recovery
Madam A had several risk factors. We encouraged her to eat fewer calories and move more. She began jogging and brisk walking for 30 minutes each morning. She also cut back on snacks and alcohol.
After three months, her liver tests returned to normal, and she reduced her weight to 60 kg.
Hepatitis B
Case Example — Madam B
Madam B was referred by her obstetrician after testing positive for the hepatitis B surface antigen (HBsAg) during pregnancy. She felt anxious about passing the virus to her baby. Her mother had cirrhosis caused by hepatitis B, and one of her brothers was also a carrier. She had never been tested until now.
Prevalence and Transmission
Around 3.6% of adults in Singapore have chronic hepatitis B. Globally, the World Health Organization (WHO) estimated 296 million people lived with the virus in 2019, with 1.5 million new cases each year. In 2019, hepatitis B caused about 820,000 deaths, mostly due to cirrhosis and liver cancer.
Hepatitis B spreads most often from mother to baby during birth or through blood contact in early childhood. It can also spread through needle injuries, tattooing, piercings, transfusions, or unprotected sex.

Prevalence and Transmission
About 3.6% of adults in Singapore live with chronic hepatitis B. Globally, the WHO estimates 296 million people had chronic infection in 2019, with 1.5 million new cases each year. In 2019, hepatitis B caused around 820,000 deaths, mainly due to cirrhosis and liver cancer.
Hepatitis B spreads most often from mother to child during birth or through contact with infected blood in early childhood. It can also spread via needle injuries, tattooing, body piercings, blood transfusion, or unprotected sex.
Pregnancy Care
We reassured Madam B that the baby was safe during pregnancy. Tests showed a high viral count but normal liver function. To reduce the risk of transmission, she started antiviral treatment in her third trimester.
She later delivered a healthy baby boy. The newborn received hepatitis B immunoglobulin and vaccine at birth. Follow-up tests confirmed the baby was virus-free and had developed protective antibodies.
Madam B continues regular blood tests and ultrasounds to watch for complications such as cirrhosis or liver cancer. She also encouraged her family members to get screened.
Autoimmune Hepatitis
Case Example — Madam C
Madam C came to my clinic after her family doctor found abnormal liver test results. The doctor had already ruled out common causes such as hepatitis B, hepatitis C, and fatty liver. Madam C exercises regularly and does not drink alcohol.
Further tests showed elevated immunoglobulin levels and autoantibodies. A liver biopsy confirmed autoimmune hepatitis.
Understanding the Disease
Autoimmune hepatitis is less common than fatty liver or hepatitis B, but it affects more women than men. It occurs when the immune system attacks liver cells, often triggered by infections, medications, or unknown factors.
Treatment and Concerns
Doctors usually treat autoimmune hepatitis with medicines that suppress the immune system, such as steroids and azathioprine.
Madam C worried about steroid side effects like weight gain, high blood sugar, and osteoporosis. We prescribed a steroid with fewer body-wide effects and added azathioprine. Over three months, her liver tests improved. We gradually stopped steroids, and now she maintains good health with azathioprine alone.
Liver Diseases in Pregnancy
Case Example — Madam D
Madam D, 28 weeks pregnant, saw her dermatologist for intense itching on her palms and soles. The discomfort kept her awake at night. Until then, her pregnancy had been smooth, and she had no history of liver problems. The dermatologist suspected intrahepatic cholestasis of pregnancy (ICP) and referred her to me.

Understanding ICP
Pregnancy brings many physical and hormonal changes. Some can trigger liver problems. Doctors must check if liver issues are pre-existing or pregnancy-related.
ICP is the most common liver disease during pregnancy. Its cause is unclear but may involve genetic factors, gallstones, fatty liver, or hepatitis C infection.
Diagnosis and Management
In Madam D’s case, itching on the palms and soles helped differentiate ICP from other skin conditions. Blood tests showed raised bile acids and mildly abnormal liver results.
We prescribed medication to reduce bile acids and relieve itching. Madam D improved and could sleep better. Her obstetrician closely monitored her baby’s health. She later delivered a healthy baby girl at 37 weeks.
Conclusion
Liver health plays a critical role in women’s overall well-being. Recognising symptoms early and seeking medical care helps prevent complications.
A balanced diet, regular exercise, and limiting alcohol can reduce the risk of many liver disorders. Staying proactive with screenings and healthy habits protects long-term liver health. PRIME








Leave A Comment