

Shoulder Bolster
A Comprehensive Guide to Understanding and Managing Unexplained Front Shoulder Pain

Shoulder pain is a prevalent and complex condition within the realm of musculoskeletal pain. The shoulder complex is a remarkable structure that enables a wide range of movements, including 360 degrees of motion that is powered by strong muscles, exceptional flexibility and impressive strength. However, this intricate design also renders the shoulder susceptible to various iniuries and conditions, leading to shoulder pain.
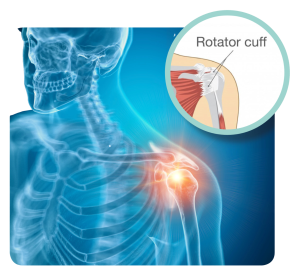
Among the many sub- types of shoulder pain, shoulder tendon degeneration and tears stand out as the most common. The rotator cuff is a group of small muscles and tendons in your shoulder that work together to help you lift and rotate your arm (see Figure 1)
The rotator cuff plays an essential role in stabilising your shoulder joint and allowing you to perform various arm movements, such as reaching and lifting objects.
Rotator cuff-related shoulder pain (RCRSP) has become a prominent clinical term encompassing a spectrum of shoulder pain related to rotator cuff tendon and adjunct tissue disorder.
This condition has a lifetime prevalence range of between 18-31% in the general population.
In this article, we will delve into the complexities of shoulder pain and explore the role of physiotherapy in diagnosing, managing and rehabilitating individuals with RCRSP.
We will discuss the underlying causes of shoulder pain, the importance of early intervention and the various physiotherapy approaches aimed at optimising shoulder function and improving overall quality of life.
CLINICAL PRESENTATION
One of the defining features of RCRSP is its traumatic nature, meaning it can arise without any specific traumatic event. It can affect individuals across different age groups and activity levels. In athletic youth and adults, overuse of the shoulder is often a contributing factor. Activities such as repetitive throwing, overhead movements in sports and weightlifting can put excessive strain on the rotator cuff tendons, leading to pain and discomfort.
On the other hand, RCRSP can also manifest spontaneously in the senior population due to age-related changes in the shoulder structures. As we age, the tendons of the rotator cuff may become more susceptible to degeneration, becoming stiffer and weaker which makes them prone to injury, even with minimal stress.
The primary complaint of individuals with RCRSP is localised shoulder pain, often in the front. The pain may worsen with certain movements, especially when the arm is raised in an overhead position or extended behind the back. In addition to pain, weakness is a common symptom associated with RCRSP. Patients may find it difficult to perform tasks that require arm strength, such as lifting heavy objects or reaching for items on high shelves. This weakness can further affect the individual’s ability to engage in daily activities and may lead to functional limitations.
Another aspect that is often affected by RCRSP is sleep. Many individuals with this condition report difficulty sleeping on the affected shoulder due to pain and discomfort. As a result, their sleep patterns may be disrupted, leading to fatigue and reduced overall well-being.
CAUSES AND MECHANISM
The exact causes and underlying pathology of RCRSP are not yet fully understood. However, research has shed some light on potential factors contributing to this condition. In the young and athletic population, RCRSP is often suggested to be related to overuse. Athletes involved in activities that require repetitive overhead movements, such as swimmers and racket sports players, are more prone to developing RCRSP.
With their arms often taking on overhead positions during these sporting activities, there is more stress placed on their rotator cuff tendons. The repetitive movements can lead to microtrauma, and gradual wear and tear, eventually resulting in pain and inflammation in the shoulder joints.
In contrast, the senior population may experience RCRSP due to degenerative changes in the tendon, even if they do not perform much overhead activities. With age, the tendons naturally undergo a reduction in blood supply and collagen content, making them more susceptible to injury and degeneration. As a result, the tendons become less resilient and more prone to inflammation, leading to shoulder pain.
Researchers have found increased levels of certain inflammatory substances in individuals with RCRSP, such as Vascular Endothelial Growth Factor (VEGF), Interleukin-1 (IL-1), and Interleukin-6 (IL-6). These inflammatory substances are associated with tissue damage and the body’s response to injury. Interestingly, the levels of these substances have been shown to correlate with the level of pain experienced by patients, indicating their involvement in the pain pathway.
Thus, RCRSP in the senior population can be attributed to a combination of degenerative changes and inflammation within the shoulder tendons.
ASSESSMENT
Diagnosis of RCRSP often requires the expertise of an orthopaedic specialist, who will perform a comprehensive examination. In more complex or severe cases, an MRI may be necessary to differentiate the condition from other similar shoulder issues or to detect any tendon tears that may require surgical repair.
Physiotherapy also plays a crucial role in clinical assessment. As physiotherapists, we will carefully assess various aspects of the shoulder, including the location of pain, the strength of each tendon in specific positions, the quality of movement of the shoulder joint, and the scapula’s movements. We will also evaluate both painful and non-painful ranges of motion to gain a comprehensive understanding of the shoulder’s condition.
HOME MANAGEMENT
Home management plays a crucial role in the overall recovery process for individuals with RCRSP. While clinical management provides essential guidance and treatment during physiotherapy sessions, the majority of the healing process occurs outside the clinic. Proper home management is essential to ensure faster healing, prevent further aggravation of the condition, and promote long-term shoulder health.
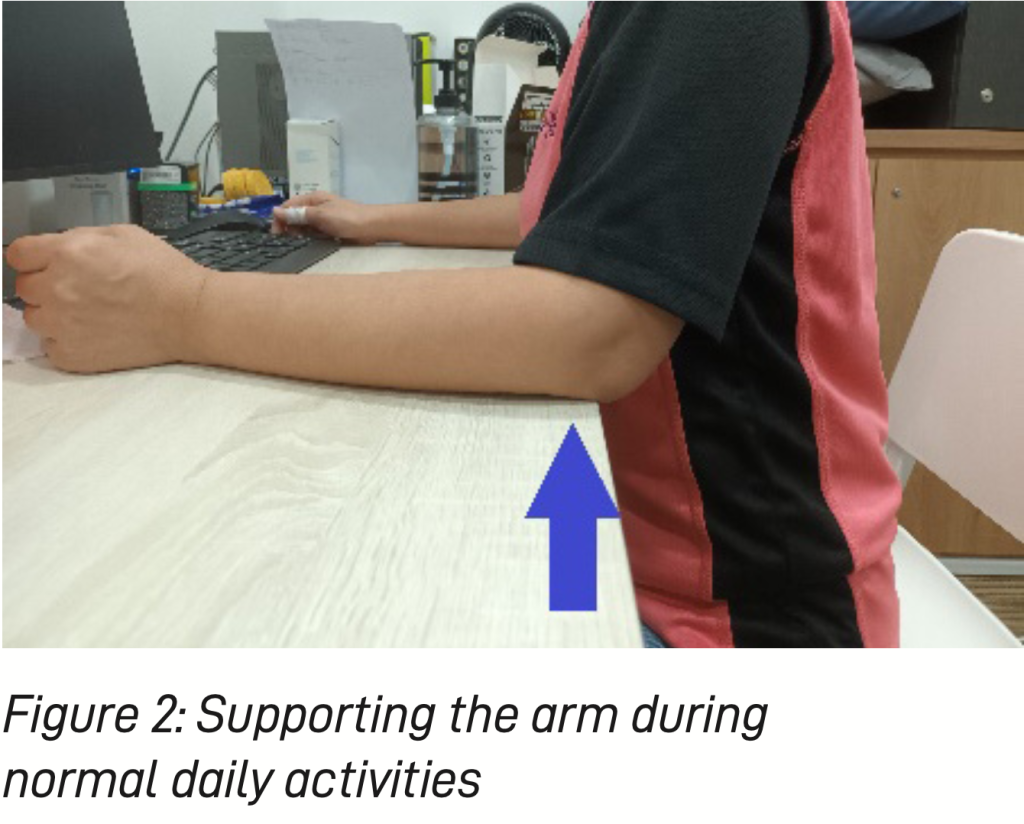
One of the primary goals of home management is to avoid activities that may trigger pain and discomfort. A physiotherapist will educate the patient on identifying and steering clear of movements or positions that strain the shoulder. For instance, in cases of pain, it is advisable to provide support to the arm most of the time, even during normal daily activities and rest (see Figure 2). By minimising the weight of the arm pulling on the affected tendon, patients can reduce pain and allow the shoulder to heal more effectively.
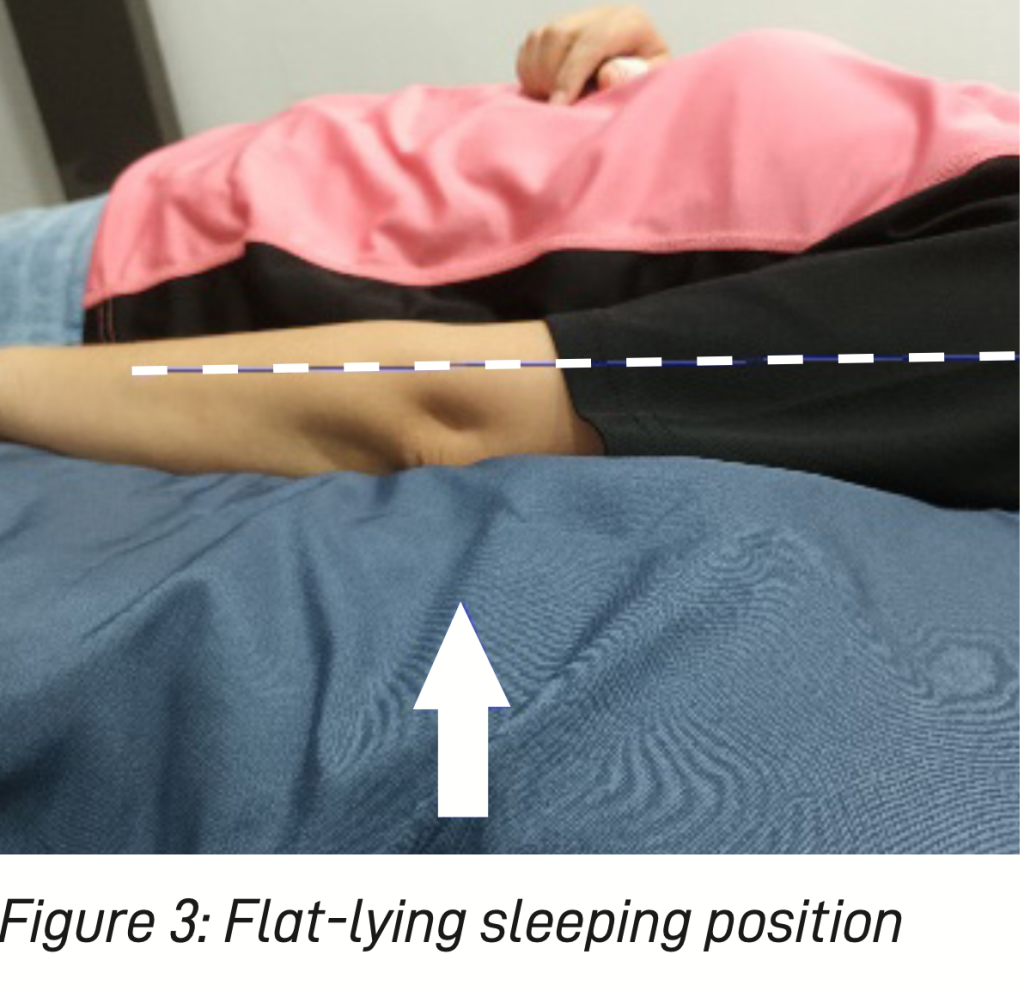
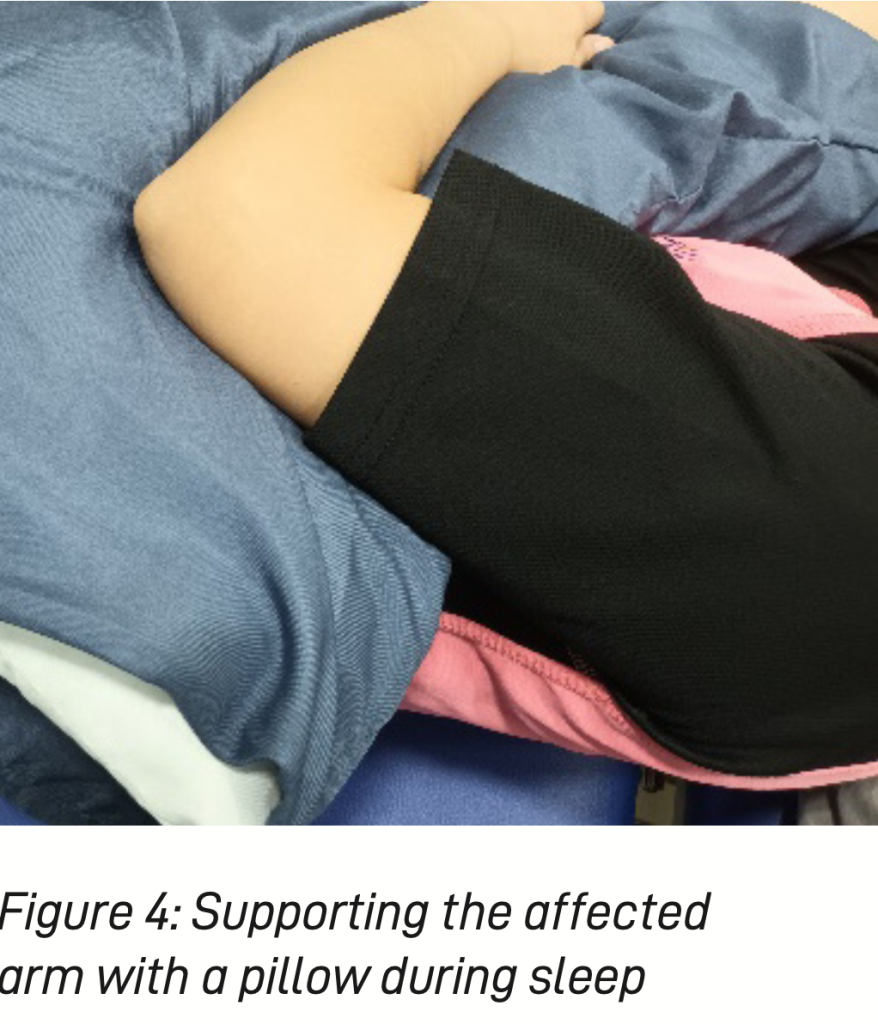
During sleep, the choice of the sleeping position is crucial for individuals with RCRSP. To avoid undue pressure on the shoulder, it is recommended to lie flat or on the non-painful side while supporting the affected arm with an extra pillow (see Figures 3 and 4). This position helps to maintain a neutral alignment and reduces strain on the shoulder joint, facilitating more restful sleep. In addition to proper sleeping positions, patients should be cautious when lifting heavy objects. Straining the shoulder during heavy lifting can worsen the condition and delay healing.
It is essential to seek help or use alternative methods when faced with lifting tasks that could strain the shoulder.
Maintaining non-painful activities is an essential aspect of home management. Staying active while avoiding activities that exacerbate pain helps to promote blood flow and basic metabolism, which are vital for healing. Patients are encouraged to continue activities involving the elbow and forearm without stressing or stretching the shoulder excessively.
CLINICAL MANAGEMENT
While education remains the cornerstone of managing this condition, various clinical interventions can also significantly contribute to a patient’s recovery. One of the most common clinical treatments is electrotherapy, which involves the use of electrical stimulation for pain relief.
This non-invasive technique helps to alleviate discomfort by stimulating the nerves and reducing pain signals sent to the brain. Additionally, ultrasound therapy is also commonly employed to target the affected area with sound waves, which promotes blood flow and accelerates the healing process. In some cases where there is remarkable tendon degeneration, extracorporeal shockwave therapy may be utilised. This technique utilises strong, localised mechanical impulses to stimulate the body’s natural healing response and encourage
tissue repair.
Another essential aspect of clinical management is manual therapy, which involves the application of hands- on techniques by the physiotherapist. In the context of RCRSP, manual therapy typically focuses on soft tissue release in the biceps and shoulder posterior capsule. These techniques aim to reduce muscle tension and tightness in the affected areas, which can contribute to pain and a limited range of motion. By releasing tension and restoring normal tissue mobility, manual therapy helps to improve shoulder function and provides relief from discomfort.
Manual therapy and electrotherapy can be effective in providing short-term pain relief, enabling patients to perform therapeutic exercises with reduced discomfort.
Other than these forms of clinical management, exercise is arguably the most crucial component for achieving long-term improvement in RCRSP. Exercise not only helps one to regain non-painful movements and restore strength, it also plays a pivotal role in promoting tissue healing and overall recovery.
Traditionally, specific strengthening exercises for the rotator cuff and scapular muscles have been prescribed to target the affected areas. Recent research has demonstrated that general shoulder strengthening exercises can be similarly effective. The ideal exercise programme is tailored and prescribed by a physiotherapist, taking into account the individual’s condition and symptoms. During exercise, it is essential to ensure that there is little to no pain, and that pain levels do not increase during or after the exercise. Targeting the weak muscles is crucial to enhancing shoulder stability and function.
The progression of exercises should be safe and follow the stages of tissue healing. This includes gradual increases in resistance, as well as changes in exercise positions and complexity. For example, as the symptoms decrease, exercises can progress from arm-neutral positions to elevated and overhead positions. The aim is to challenge the muscles progressively and resume the pre-injury functions, while ensuring that the exercises remain within a pain-free range.
Safe progression is critical to avoiding injury aggravation and promoting healing.
The benefits of exercise extend beyond simply improving flexibility and muscle strength. Scientific research has shown that resistance training can induce the secretion of mechanically sensitive substances, such as tenocytes, Interleukin-6 and Cyclooxygenase-2, in body tissues. These substances play a role in regulating the inflammatory activities of the tissues. As a result, exercise can reduce pain and improve overall function in patients with RCRSP.
EXPECTED OUTCOME
The rate and degree of recovery in rotator cuff-related shoulder pain can vary significantly based on several factors, including age, lifestyle, general health and the effectiveness of management.
For young adults with overuse-related RCRSP, the recovery process may be faster as their bodies tend to respond well to treatment and rehabilitation. On the other hand, older adults with degenerative RCRSP may experience a slower recovery due to age-related changes in tissues and healing capacity. In such cases, the management process may take up to a year to achieve optimal results. In more severe cases of RCRSP, such as those involving tendon tears, surgical repair may be necessary. Following surgery, a comprehensive rehabilitation programme spanning several months is typically required to fully restore function and strength.
To achieve the best possible outcomes, early detection of RCRSP is crucial. Timely intervention can prevent the condition from worsening and may lead to quicker recovery. A comprehensive management plan, including physiotherapy, exercise and lifestyle adjustments, is essential to promote healing and reduce the risk of recurrence.
Compliance with self-care advice is equally important throughout the recovery process. Patients should follow their clinicians’ recommendations diligently, including adhering to prescribed exercises and avoiding activities that exacerbate pain.








Leave A Comment