

Understanding Esophageal Cancer: Symptoms, Diagnosis, Treatment and Prevention
The oesophagus (pronounced as ee-so-fa-guhs) – also called the food-pipe or gullet – is a muscular tube connecting the back of the throat to the stomach.
It is about 25cm long and runs downwards from the throat, behind the airway (trachea) and the heart in the chest, and passes through the diaphragm to connect to the stomach.
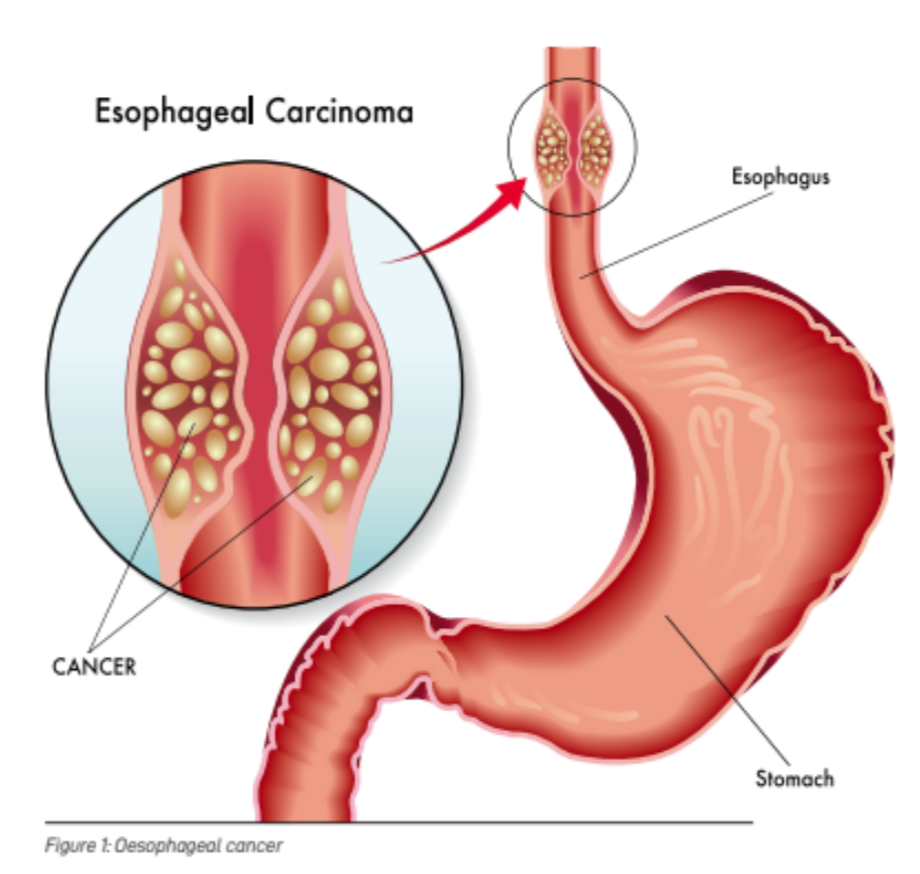
Its main function is to carry food and liquid from your mouth into the stomach.
At the top and bottom of the oesophagus are the upper and lower oesophageal sphincter muscles that stop food and liquid from refluxing up from the stomach into the oesophagus (thereby causing heartburn/indigestion) or into the throat.
OESOPHAGEAL CANCER
Oesophageal cancer (OC) is associated with a poor prognosis. Globally, OC remains a major cause of cancer mortality and disease burden. It is the 8th most common cancer and the 6th leading cause of cancer death worldwide. About half a million new oesophageal cancer cases occur annually and 75% of these are in Asia.
OC accounts for an estimated one in every 20 cancer-related deaths (GLOBOCAN). Men are three times more likely to get OC than women, and OC tends to occur after the age of 50.
According to the Singapore Cancer Registry, it is the 10th most frequent cause of cancer death in men in Singapore.
SYMPTOMS
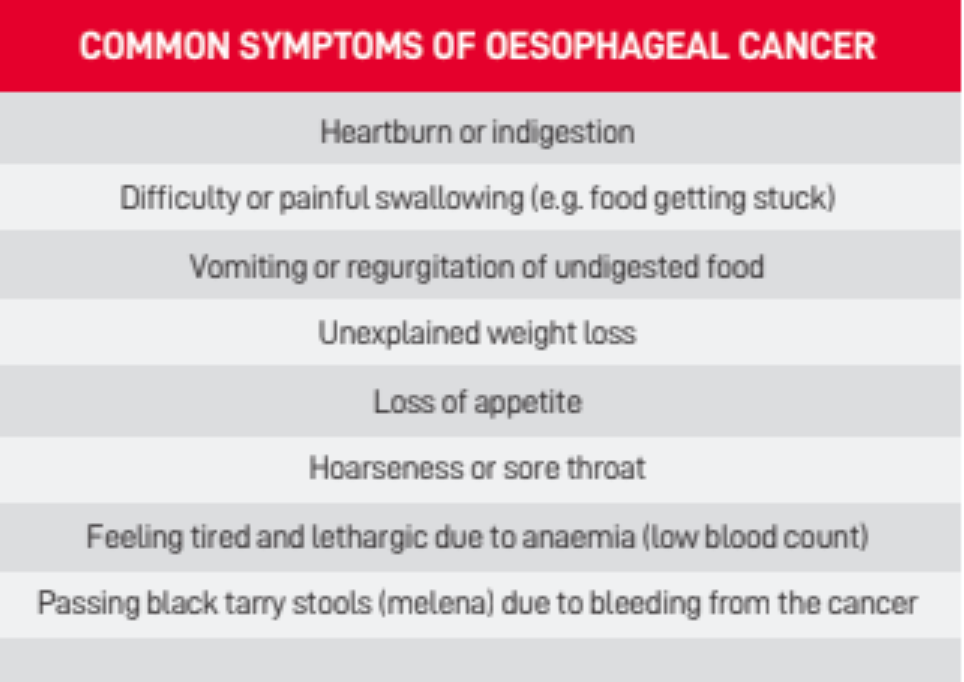
The symptoms of OC can range from no symptoms (when the cancer is very early) to vague non-specific symptoms, to more alarming symptoms of difficulty in swallowing and unexplained weight loss.
The latter often indicates a late cancer stage. Hence, there is a need for early detection of this cancer.
A national public education programme to raise public awareness would certainly help. At the early stage, the symptoms of OC are non-specific. In most cases, these symptoms can mimic benign diseases like gastro- oesophageal reflux disease (GORD). Patients with GORD will also have chronic heartburn or indigestion, chest pain, coughs,sore throat and even difficulty in swallowing. Hence, it is easy to ignore these early symptoms and attempt to self-medicate with over-the-counter drugs like antacids. As a result, OC patients often present too late in 70% of cases, whereby the five-year survival rate is less than 5%.
TYPES OF ESOPHAGEAL CANCER
There are two main types of esophageal cancer, namely oesophageal squamous cell carcinoma (SCC) and adenocarcinoma (OAC). They have very distinct risk factors and geographical distributions.
Oesophageal SCC accounts for 90% of all oesophageal cancer cases globally. It is the predominant type in Asia, Africa, and South America. On the other hand, OAC is the predominant type of OC in the western world, especially in North America and western Europe.
ESOPHAGEAL SCC
SCC arises from long-standing irritation (and inflammation) of the esophageal lining, most commonly due to smoking and alcohol abuse. They act synergistically to develop SCC. While tobacco and alcohol consumption are the major risk factors for esophageal SCC in many parts of the world, they are not strong risk factors in the Asian esophageal cancer belt. Studies have found that consumption of very hot tea, low intake of fresh fruits and vegetables, indoor air pollution, lack of access to clean water, poor oral health, and low socioeconomic status are associated with a higher risk of SCC in Asia.
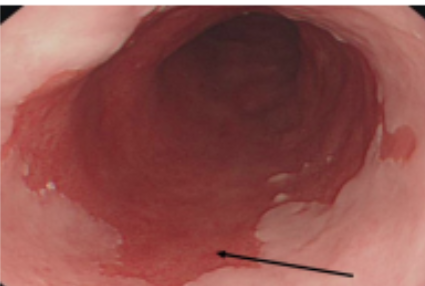
Figure 2. Barrett’s oesophagus (arrow) is a precancerous condition which develops from chronic gastro-cesophageal rettux disease
BARRETT’S ESOPHAGUS AND OESOPHAGEAL ADENOCARCINOMA
The incidence of OAC has risen by over 500% in the past 4 decades, especially in white males. It is linked to the increasing prevalence of chronic acid reflux (gastro-oesophageal reflux disease) and obesity. Barrett’s esophagus (see Figure 2) is a precancerous condition where the lining of the lower esophagus changes to adapt to the chronic acid reflux (gastro-oesophageal reflux disease).
The acid damages the lining and the lining changes into Barrett’s esophagus. Such patients need endoscopic surveillance. In a small proportion of people (0.5-1%), the Barrett’s esophagus will undergo transition from low-grade or high-grade to OAC.
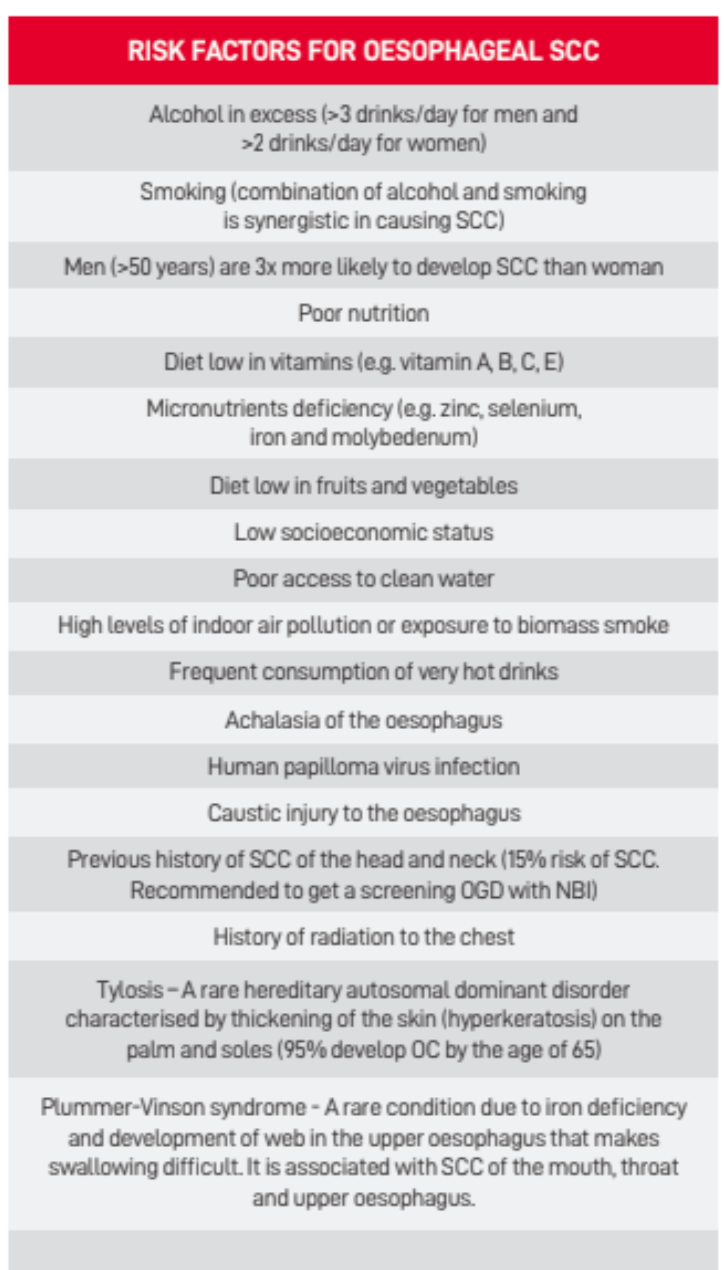
Table 2: Risk factors for esophageal SCC
Given the poor survival rate of patients with OC, major efforts to reduce these risk factors should be undertaken. This is especially so given that many risk factors (e.g. smoking, alcohol and obesity) also contribute to other major chronic diseases like cardiovascular diseases, diabetes and other cancers.
DIAGNOSIS
OC is diagnosed with an oesophago-gastro-duodenoscopy (OGD). During this simple 10-minute examination which is performed under sedation, a small flexible telescope is inserted through the mouth into the esophagus, stomach, and duodenum. This test is performed using white light and a virtual chromoendoscopy technique known as narrow band imaging (NBI). It highlights any abnormal areas (precancerous areas or cancer) that may be treated endoscopically.
ENDOSCOPIC RESECTION
When precancerous lesions or very early cancer is found, they can also be removed with a technique called endoscopic resection (ER – see Figure 3).

Figure 3: Endoscopic mucosal resection for precancerous lesions or very early cancer
ER is a minimally invasive technique to treat and remove very early OC (intramucosal/T1a and some T1b cancers). This technique is performed with the use of OGD through the mouth.
It is safe and curative, and is performed as a day procedure under sedation. If the final histology proves to be very early OC or precancerous lesions, there is no need to undergo a major complex surgery (e.g. oesophagectomy) which comes with all its risks up-front.
This allows the patient to recover faster with less pain and enjoy a better quality of life as compared with patients who have had an oesophagectomy.
RADIOFREQUENCY ABLATION (RFA) AND ARGON PLASMA COAGULATION (APC)
RFA is an endoscopic ablative procedure performed under sedation or general anaesthetic to eradicate the precancerous lining of the esophagus (e.g. low or high-grade dysplasia, or Barrett’s). It works by burning away the lining in a controlled fashion. This technique is only used to treat precancerous areas that are flat (any nodular lesion will need prior removal by ER to ensure that it is not a cancer).
RFA is approved for use in Barrett’s with low or high-grade dysplasia, or those who have Barrett’s and a strong family history of OAC. It is used to burn all the flat Barrett’s away to reduce the risk of cancer development. Smaller areas of flat precancerous lining can be treated by APC to burn them away.
APC is a cheaper and easier technique, but it is only used to treat smaller areas (e.g. <2cm of Barrett’s).
RFA has been proven in rigorous clinical trials to be safe, cost- effective and successful in eradicating the precancerous lining (e.g. Barretts with dysplasia or squamous dysplasia) in over 98% of cases. In turn, this helps to prevent the development of OC. Long term follow-up (5 years) of the trial patients proved RFA to be durable and safe.
Early detection of OC is appealing because precancerous lesions and very early cancers can be treated effectively with OGD, such as ER, RFA and APC. In some areas of China where there are high incidence rates of SCC and its precursor lesions (squamous dysplasia), mass upper gastrointestinal endoscopy screening has been shown to increase survival rates, while also being highly cost effective.
Early detection of OC can also occur as a by-product of screening for gastric cancer. For example, in South Korea and Japan, mass screening for gastric cancer using OGD is done as part of a national screening programme. This screening has helped in the early detection of esophageal cancer.
On the other hand, due to its low progression rates, population screening for Barrett’s oesophagus to prevent OAC is not cost effective.
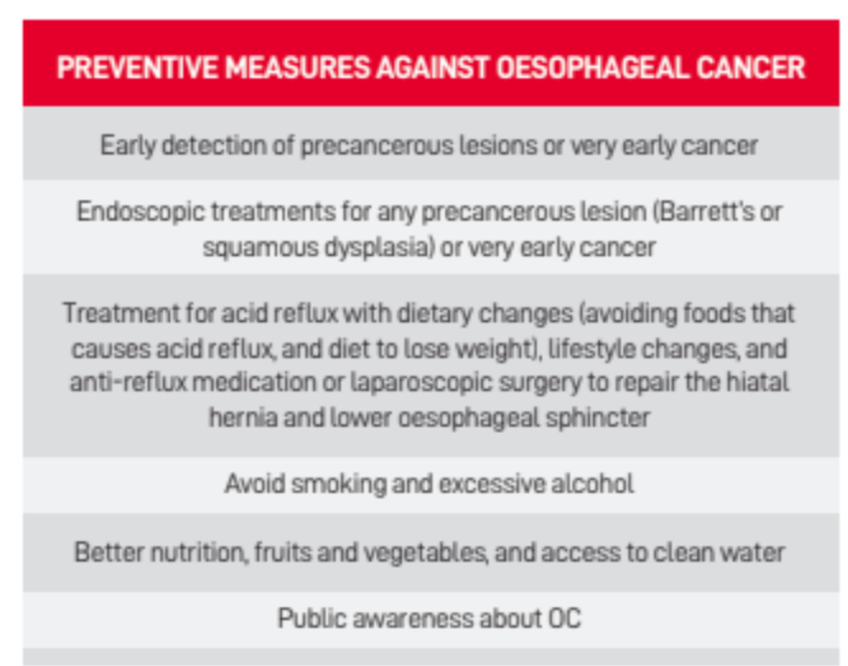
Table 4: Preventive Measures Against Oesophogeal Cancer
PREVENTION
Can esophageal cancer be prevented? Yes, to some extent. Table 4 illustrates some of the actions that can prevent OC.
TREATMENT FOR LOCALLY ADVANCED OESOPHAGEAL CANCER (STAGE 2 OR 3)
Oesophageal cancerat stage 2 or 3 often needs a multimodality treatment which includes surgery (including MIO and RAMIO), chemotherapy and/or radiotherapy. Currently, surgery is still the cornerstone of curative therapeutic modality. However, its applicability is restricted to the earlier stages of OC. Oesophagectomy remains a challenge even with current advances (such as robotic surgery), because the oesophagus spans three anatomic compartments: the neck, the thorax and the abdomen. Its proximity to vital structures like the trachea, bronchus, heart and aorta poses another major challenge.
MINIMALLY INVASIVE AND ROBOTIC OESOPHAGECTOMY
The pioneering of minimally invasive oesophagectomy (MI0) by US Professor James D. Luketich has revolutionised oesophageal cancer surgery, with the use of laparoscopic and thoracoscopic equipment (key-hole surgery see Figure 4). Over the last 2 decades, MIO has expanded worldwide. Its use has facilitated faster patient recovery with less pain and less blood loss for patients.

Figure 4: Minimally invasive pesophagectomy
This technique has also proven to be equal to open cancer surgery in terms of outcome. However, MIO is a complex major operation, and takes longer to learn and to perform.
Robotic assisted minimally invasive oesophagectomy (RAMIO) is another form of minimally invasive surgery. The surgeon controls the arms of the robot while being seated at a computer console near the operating table (see Figure 5). The robot gives the surgeon a stable, high definition 10x magnified 3D view of the surgical site.
The instruments have seven degrees of articulations, culminating in a highly precise surgery even in hard-to- reach areas. The main downside of RAMIO is the cost of the robot. But this should improve in the future to provide better healthcare for more people.
RAMIO is a win-win-win situation for healthcare. It is a win for patients because of the better technology and outcomes. It is also a win for surgeons because of the better ergonomics when they are performing a long complex operation. This translates to less fatigue, back, neck or shoulder injury for the surgeons.
Furthermore, it is also a win for medical institutions because their patients will have better outcomes and higher quality operations, while their experienced surgeons can put in more high-quality operating hours during their careers because they will require less time off work from fatigue or injury.

Figure 5: Robotic assisted minimally invasive oesophagectomy with surgeon sitting at the console (next to the patient) and controlling the arms of the robot
CHEMOTHERAPY
Chemotherapy uses anti-cancer drugs to destroy cancer cells. The drugs circulate in the bloodstream throughout the body. For stage 2 or 3 0C, a combination of 2-4 drugs is given intravenously and/or orally for 3-4 cycles over three months. These drugs can be given before and after surgery (peri-operative chemotherapy); before surgery (neoadjuvant chemotherapy); or after surgery (adjuvant chemotherapy). Sometimes, they are given in combination with radiotherapy before surgery (neoadjuvant chemoradiation).
The aim of these treatment regimens is to reduce the size of the cancer and to reduce the risk of cancer recurrence after surgery. However, there are side-effects to chemotherapy.
These include nausea, vomiting, diarrhoea, lethargy, weight loss, hair loss, infection, hand-foot syndrome and neuropathy. Most of these side-effects disappear when the treatment is completed. Well-conducted phase 3 randomised controlled clinical trials (RCT) have shown a significant improvement in survival with peri-operative chemotherapy for 0C (e.g. FLOT4,
MAGIC) when compared with patients who had surgery alone. In 4 stage 4 cancer, when the cancer cells have spread to other organs (e.g. metastatic liver cancer), palliative chemotherapy is given to shrink these cancers and to relieve symptoms. It will not be curative, but it allows the patient to live longer.
RADIOTHERAPY
Radiotherapy uses high-energy rays (like x-rays) to kill cancer cells. It can be used alone, or in combination with chemotherapy known as chemoradiation (the chemotherapy enhances the radiotherapy effects on cancer cells, but it has side-effects). Radiotherapy beams treat only a specific area (loco-regionaleffects) and are extremely effective for oesophageal SCC because the cancer is sensitive to radiotherapy.
The CROSS trial was a phase 3 RCT which showed better survival in patients given neoadjuvant chemoradiation before surgery, especially in SCC. Palliative radiotherapy can be given in metastatic cancer to relieve symptoms, including pain, bleeding or difficulty in swallowing.
IMMUNOTHERAPY
Immunotherapy is the use of drugs that helps a patient’s own immune system to destroy cancer cells more effectively. Recent clinical trials showed that immunotherapy (immune checkpoint inhibitors or PD-1 inhibitors) have improved the outlook for patients with locally advanced or metastatic esophageal cancer. These clinical trials showed that when combining immunotherapy with chemotherapy, the combined treatment improved survival by several months. The current evidence also showed that patients with residual disease after neoadjuvant chemoradiation and OC surgery will have better survival from Nivolumab immunotherapy.
CONCLUSION
Most patients with OC, on account of late onset of symptoms and a consequential delay in the diagnosis, present with metastatic disease which precludes definitive surgical intervention. Hence, the prognosis remains poor. Early diagnosis is vital for the optimal management of OC. PRIME








Leave A Comment