

Temporomandibular Joint Disorder (TMD) and Its Physiotherapy Management
Temporomandibular joint disorder (TMD) is a muscular or articular disorder of the jaw. It usually causes jaw pain, deviation and a clicking sound. The articulation of the human jaw consists of two pieces of bone, namely temporal (side of the skull) and mandibular (lower jaw). This joint allows opening and closing of the mouth as well as other jaw movements, such as gliding forward/backward and sideways.

An articular disc slides forward and backward between the two bones during movements of the mouth to reduce friction. Biting force is generated by the oral and facial muscles on the left and right sides of the jaw. The molars of humans can exert a biting force of up to approximately 120kg. The biting force on the left and right can be different. The imbalance of the biting force during daily activities, such as chewing hard and tender foods, can cause jaw deviation. Other factors, such as trauma, overuse or degeneration may also cause displacement of the articular disc or the joint, resulting in inflammation, pain and movement deviation. These are considered as TMD. As the position of temporomandibular is right next to the auditory canal, some patients may also experience earache.
According to clinical studies, the prevalence of TMD ranges from 10-30% in different populations. Having said that, the symptoms in some cases can be very mild and patients may recover spontaneously. These cases can go unnoticed. For example, some people may occasionally feel the jaw clicking when eating or talking, but the jaw has normal function otherwise and there is no pain.
In severe cases, patients may experience significant jaw and facial pain, have no strength when chewing, and experience difficulty in yawning. Females as well as people having bruxism, stress and those doing heavy computer work are more likely to suffer from TMD.

A TMD Case Study
For the rest of this article, I will use photographs from a case study of physiotherapy management in TMD (commonly known as jaw pain) to illustrate how treatment for this condition can be done.
In this case, a female patient was initially referred to my clinic because of her neck pain. Besides her neck pain, she also complained of earache on her right side and jaw pain, which annoyed her for a period of time.
A summary of her symptoms includes the absence of dizziness and tinnitus, headache on the same side as the earache, and jaw pain. She reported receiving a dental procedure one year ago and deduced that was when her problems gradually started. For this patient, I proposed a course of physiotherapy treatment that would help to resolve her neck pain and jaw pain.

Clinical Assessment
Temporomandibular disorder is a complex condition that involves the face, jaw and neck. The first clinical assessment is usually observation. This involves imagining a line joining the forehead, nose, and middle of the patient’s mouth. A comparison for any asymmetry is then made between the left and right side of the patient’s face.
Mild facial asymmetry is usually expected in the case of TMD. Incomplete closure or opening of the mouth is another possible symptom of TMD. Further to these, normal opening movement of the mouth should measure approximately 3 finger widths of the patient (see figure 1). Patients with TMD may experience restrictions in opening their mouths due to misalignment or blockage of their jaws.

Figure 1: Observation of jaw movement during mouth opening
In addition, any clicking or jaw deviation during opening and closing of the mouth should be noted. Palpation (the therapist uses the hand to press and find the painful site) of the joint can be conducted on the ear canal, the face (see figure 2) and intraorally. Some important oral muscles between the oral cavity and outside the teeth should be checked. The tendon of an important oral muscle – the lateral pterygoid – also needs to be checked intraorally. This is because this muscle attaches to the jaw directly. Excessive tension on this muscle is a possible cause of TMD.

Figure 2: Check for pain in the temporomandibular joint
Last but not least, the first three segments of the cervical spine (neck) have a critically close connection with the jaw. In physiotherapy assessment, it is necessary to check for mobility and pain in the upper cervical spine for patients with TMD. Also, in some cases, the associated headache could be due to irritation from the upper cervical spine.
There are several conditions which share similar symptoms to TMD. These include trigeminal nerve pain, facial palsy, ear infection and dental problems. A comprehensive assessment is critical to ensure that proper treatments are prescribed. Therefore, doctors, dentists and physiotherapists have to work closely together to provide appropriate management for individual patients.
Treatment and Effectiveness
Physiotherapy management of TMD can help to reduce jaw pain and improve jaw movement during opening or closing of the mouth. Manual therapy is the key treatment for TMD. It is a direct mechanical treatment applied through the hands of physiotherapists to the joint and tissue to relieve pain and improve mobility. Typical treatments include manual mobilization to the temporomandibular joint, soft tissue mobilization on tight facial or oral muscles, and spinal manipulation to the neck (see figures 3-5).
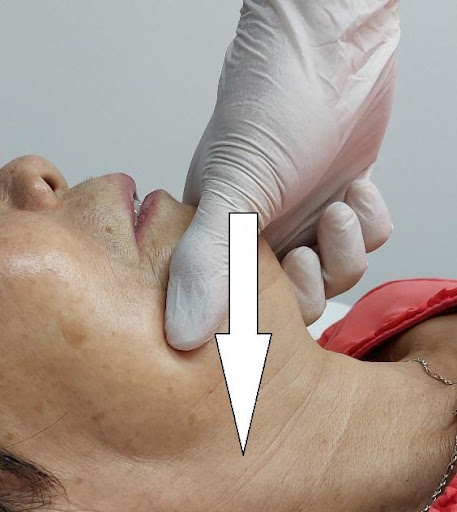
Figure 3: Manual treatment to the joint – backward direction

Figure 4: Manual treatment to the joint – forward direction

Figure 5: Spinal manipulation to the neck
Home exercise prescriptions for the chewing muscles and neck muscles are also important for long term benefit. Patients will be taught to perform simple exercises at home to strengthen their neck muscles, which help to stabilize their neck and jaw positions. Self-massage to the facial muscles can help to reduce excessive tension. Also, specific exercise training for the chewing muscles can balance the force between the two sides during daily activities.
Prognosis
The prognosis of TMD is usually optimistic as long as patients realize their condition and seek early treatment. In some cases, if the joint clicking is severe, it may indicate significant articular disc displacement. In these cases, the management may be more complicated.
Comprehensive clinical research has shown that manual therapy is effective in reducing pain and improving jaw movement for patients with TMD. When complemented with therapeutic exercise, the treatment effects can be maintained long term.
Author

You Might Also Like:
 Reclaim Shoulder Supremacy: Uncover Rotator Cuff Recovery Tips! by Christopher Lo Chi Ngai
Reclaim Shoulder Supremacy: Uncover Rotator Cuff Recovery Tips! by Christopher Lo Chi Ngai
 Getting the Needle by Christopher Lo Chi Ngai
Getting the Needle by Christopher Lo Chi Ngai
 Pilates & Physiocare: The Perfect Combination for Various Therapeutic Functions by Mr John Abraham
Pilates & Physiocare: The Perfect Combination for Various Therapeutic Functions by Mr John Abraham
 Advances in Retinal Disease Treatment by Dr Leonard Ang
Advances in Retinal Disease Treatment by Dr Leonard Ang
 Defeating Cavities by Dr Raymond Lim
Defeating Cavities by Dr Raymond Lim


Leave A Comment